On July 10, 2024, the Centers for Medicare and Medicaid Services (CMS) issued the 2025 Medicare Hospital Outpatient Prospective Payment System (OPPS) Proposed Rule (link) with an accompanying fact sheet (link).
Proposed Rule highlights include:
For CY 2025, CMS proposes to increase OPPS payment rates for hospitals and ambulatory surgical centers (ASCs) that meet quality requirements by 2.6 percent (a 3 percent market basket increase blended down by a 0.4 percent productivity adjustment).
Payment for Devices/Drugs in a Clinical Trial with a Medicare Coverage with Evidence Development (CED) Designation: For CY 2025, CMS proposes to develop alternative methods of payment under Medicare Part B for drugs and devices being studied in clinical trials under a CED National Coverage Decision (NCD).
Cell and Gene Therapy: For CY 2025 only, CMS proposes not to package payment for certain cell and gene therapies into the payment for the primary Comprehensive Ambulatory Payment Classification (C-APC) service when they appear on the same claim as primary C-APCs services.
HIV Pre-Exposure Prophylaxis (PrEP): For CY 2025, CMS proposes to pay for HIV PrEP drug and related services as additional preventative services under the OPPS, pending coverage in the final NCD. Additionally, CMS proposes a “site neutral policy” where products would be paid similar rates under OPPS and the Physician Fee Schedule (PFS).
Invoice Drug Pricing Proposal: CMS proposes to adopt an invoicing pricing policy beginning in CY 2026 for novel drugs and biologics which do not have sufficient Wholesale Acquisition Cost (WAC), Average Wholesale Price (AWP), sales, and Mean Unit Cost (MUC) information for CMS to assign a payable status indicator.
Comments are due on September 9, 2024.
Below, ADVI provides an overview of the Proposed Rule. Please contact your ADVI Account Manager for additional details.
Payment for Devices in Category B Investigational Device Exemption (IDE) Clinical Trials and Drugs/Devices Being Studied in Clinical Trials with a Medicare CED NCD
Payment Policy for Devices in Category B Investigational Device Exemption (IDE) Clinical Trials Policy
Background: In the CY 2023 OPPS Final Rule, CMS finalized a policy to make a single blended payment for devices and services in Category B IDE studies.
CMS notes that the goal of this policy change was to preserve the validity of these studies by avoiding differences in Medicare payment methods that would reveal the treatment or control group (e.g., if the treatment group received higher payment than the control, this would reveal which arm was which).
CMS stated that they would create, or revise an existing, HCPCS code to describe a Category B IDE study, which includes both the treatment and control arms, related devices, and routine care and services.
Further, CMS finalized that the single blended payment rate would be dependent on the specific trial protocol and account for how frequently the investigational device and control are used.
In response to stakeholder questions, in the 2025 OPPS Proposed Rule CMS clarifies that the above policy applies only to IDE studies with a control arm. CMS states that Category B IDE studies with no control arm would be paid normally as an alternative methodology is not necessary.
Payment for Drugs/Devices Being Studied in Clinical Trials with a Medicare CED NCD
For CY 2025, CMS proposes to “utilize a payment methodology similar to the one developed for Category B IDE clinical trials for drugs and devices covered under a national coverage determination (NCD) that uses the Coverage with Evidence Development (CED) paradigm and a payment adjustment is necessary to preserve the scientific validity of such a study”.
More specifically, CMS proposes to develop alternative methods of payment under Medicare Part B for drugs and devices being studied in clinical trials under a CED NCD.
CMS states that, similar to their policy on devices in Category B IDE trials, for devices under a CED NCD the agency would make a single blended rate payment dependent on the specific trial protocol and account for how frequently the investigational device and control are used.
Separately, CMS proposes to make payment using an “adjusted payment level” representing the frequency with which the study drug and placebo (or comparator) are used.
CMS proposes to base the payment amount for the study drug, or active comparator drug, on ASP plus 6 percent.
If ASP data is not available, CMS proposes to pay according to the existing payment hierarchy for non-passthrough separately payable drugs in OPPS.
CMS would use these amounts to calculate the adjusted payment level. CMS proposes to use a zero-dollar amount for a placebo or comparator.
CMS notes that a new, or revised, HCPCS code would be created for the drug and placebo or comparator in the CED study, which would be assigned to a its own Ambulatory Payment Classification (APC).
CMS notes that an alternate payment methodology for routine costs of an approved clinical would be implemented only when necessary to maintain the scientific validity of the trial (i.e., if routine costs differed between the treatment and control arms).
CMS seeks comment on other instances where Medicare payment methodologies could interfere with the scientific validity of a trial.
Exclusion of Cell and Gene Therapies from Comprehensive Ambulatory Payment Classification (C-APC) Packaging
For CY 2025 only, CMS proposes not to package payment for certain cell and gene therapies (listed below) into the payment for the primary C-APC service when they appear on the same claim as primary C-APCs services. CMS proposes this policy for one year only to gather more information as to whether this proposed policy appropriately captures all the unique therapies that function as primary treatments and do not support C-APC primary services. CMS requests comments on the potential need for a different, modified, expanded, or supplemental policy for future rulemaking and if any additional cell and gene therapies should be excluded from C-APC packaging.
Cell and Gene Therapies Proposed for Exclusion from C-APC Packaging
Yescarta
Kymriah
Provenge
Tecartus
Breyanzi
Abecma
Carvytki
Luxturna
Zolgensma
Payment for HIV Pre-Exposure Prophylaxis (PrEP) in Hospital Outpatient Departments
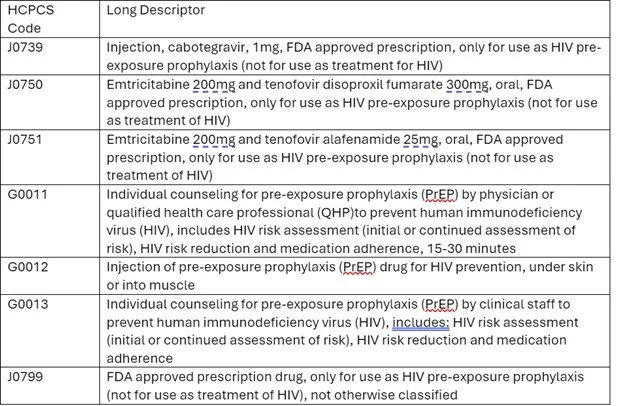
For CY 2025, CMS proposes to pay for HIV PrEP drug and related services as additional preventative services under the OPPS, pending coverage in the final NCD. CMS proposes a “site neutral policy” where products would be paid similar rates under OPPS and the Physician Fee Schedule (PFS).
CMS proposes to pay for the following HCPCS codes when furnished in hospital outpatient departments (HOPDs):
CMS proposes to utilize ASP methodology to determine the OPPS payment amount for HIV PrEP drugs.
If ASP data for HIV PrEP is not available, CMS proposes to determine the payment amount for the applicable billing and payment code using the most recently published amount for the drug in Medicaid’s National Average Drug Acquisition Cost (NADAC) survey.
If neither ASP nor NADAC data are available, CMS proposes to use Federal Supply Schedule (FSS) data.
Drug Packaging Threshold
CMS proposes to raise the threshold to $140 per day for CY 2025. This is a $5 increase from the CY 2024 threshold of $135 per day. Items with a per day cost greater than $140 are identified as separately payable unless they are policy-packaged.
Radiopharmaceuticals
Diagnostic Radiopharmaceuticals
CMS proposes the following changes to the existing policy which packages the payment of diagnostic radiopharmaceuticals with nuclear medicine tests:
Pay separately for diagnostic radiopharmaceuticals with per day costs above $630
Diagnostic radiopharmaceuticals with per-day costs equal to or below the threshold would continue to be policy-packaged
Beginning in 2026 and annually thereafter, update the $630 threshold by the Producer Price Index (PPI) for Pharmaceutical Preparations.
Base payments for separately payable diagnostic radiopharmaceuticals on their Mean Unit Cost (MUC) derived from OPPS claims (CY 2025 payments would be based on CY 2023 MUC data).
CMS seeks comments on basing payments on ASP in future years, acknowledging that because radiopharmaceuticals are not required to report ASP under Section 1847A of the Social Security Act.
Add-On Payment for Radiopharmaceutical Technetium-99m (Tc-99m)
Background: As finalized in the CY 2024 OPPS Final Rule, for CY 2025, an add-on payment of $10 will continue to apply to radiopharmaceuticals that use Tc-99 produced without the use of highly enriched uranium (HEU).
For CY 2026, CMS proposes to replace this add-on payment with an add-on payment of $10 per dose for radiopharmaceuticals that use Tc-99m derived from domestically produced molybdenum-99 (Mo-99). CMS notes that the CY 2026 OPPS Proposed Rule would include additional detail on how providers will bill for this add-on payment.
Proposed Drugs and Biologicals with Expiring Pass-Through Payment Status in 2025
There are 25 drugs and biologicals for which pass-through payment status expires by December 31, 2024 (listed in Table 62 of the Proposed Rule).
For CY 2025, CMS proposes to end pass-through payment status for 28 drugs and biologicals which were initially approved for pass-through payment status between April 1, 2022-January 1, 2023 (listed in Table 63 of the Proposed Rule). The associated ambulatory payment classification (APCs) and HCPCS codes will end by December 31, 2025. Consistent with CY 2024, CMS would continue to provide payment for pass-through drugs and biologicals for CY 2025 and beyond using the ASP methodology.
Device Pass-Through Status
CMS received 14 device pass-through payment applications by March 1, 2024, which was the deadline to be included as part of this Proposed Rule. CMS requests comments on whether these devices meet the eligibility criteria.
Alternative Pathway Device Pass-Through Applications for Breakthrough Devices
AGENT™ Paclitaxel-Coated Balloon Catheter
Aveir™ DR Dual Chamber Leadless Pacemaker System
CANTURIO™ Tibial Extension (CTE) with Canary Health Implanted Reporting Processor (CHIRP®) System
The DETOUR™ System
EndoSound Vision System™ (EVS™)
iFuse Bedrock Granite™ Implant System
Paradise® Ultrasound Renal Denervation (RDN) System
Precision GI
PulseSelect™ Pulsed Field Ablation (PFA) System
Symplicity Spyral™ Renal Denervation (RDN) System
Traditional Device Pass-Through Applications
Ambu® aScope™ Gastro
OMEZA Wound Care Matrix (OCMTM)
OPN NC
OSCAR® Peripheral Multifunctional Catheter
Changes to the List of ASC Covered Surgical Procedures
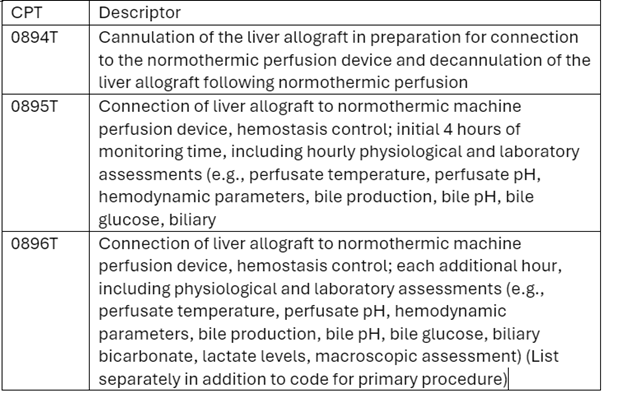
CMS proposes to update the ambulatory surgical center (ASC) covered procedures list (CPL) by adding 20 medical and dental surgical procedures to the list for CY 2025. These procedures are detailed in Table 82 of the Proposed Rule. CMS requests interested parties submit procedure recommendations to be added to the ASC CPL, particularly if there is evidence that these procedures meet CMS criteria and can be safely performed in the ASC setting. CMS notes they expect to gradually expand the ASC CPL.
Changes to the Inpatient Only (IPO) List
CMS proposes to add three new services to the IPO list in CY 2025 and to assign these services to status indicator “C” (Inpatient Only) for CY 2025. CMS does not propose to remove any services from the IPO list in CY 2024.
CMS believes the following codes meet current criteria to be added to the IPO list:
Other Notable Proposals
Invoice drug pricing proposal
CMS proposes to adopt an invoicing pricing policy beginning in CY 2026 for novel drugs and biologics which do not have sufficient WAC, AWP, sales, and MUC information for CMS to assign a payable status indicator.
Specifically, Medicare Administrative Contractors (MACs) would use the provider invoice amount to set a payment rate for separately payable drugs, biologics, or radiopharmaceuticals until their payment amount is available to CMS.
For CY 2025, impacted drugs and biologics would continue to be assigned a non-payable status indicator until the implementation of the proposed invoicing policy.
Add-on payment for high-cost drugs provided by Indian Health Service (IHS) and Tribal Facilities
For CY2025, CMS proposes to pay IHS and tribal hospitals separately for high-cost Part B drugs (daily costs over $1,334) furnished in hospital payment departments through and add-on payment in addition to the All-Inclusive Rate (AIR).
Colorectal cancer (CRC) screening
CMS proposes the following changes to coverage of CRC screening services:
Remove coverage and discontinue codes for barium enema procedures (HCPCS codes G0106 and G0120) due to the procedures no longer being recommended in clinical guidelines.
Add coverage for the computed tomography colonography (CTC) procedure (HCPCS code 74263).
Expand the existing definition of a “complete colorectal cancer screening” to include a follow-on screening colonoscopy after a Medicare covered blood-based biomarker CRC screening test (described and authorized in NCD 210.3).
CMS notes that additional details of the proposed revisions to coverage of CRC screening services are included in the CY 2025 Physician Fee Schedule Proposed Rule.
Quality measures
CMS proposes to adopt several measures across the Hospital Outpatient Quality Reporting (OQR), Rural Emergency Hospital Quality Reporting (REHQR), and Ambulatory Surgical Center Quality Reporting (ASCQR) Programs, including:
Hospital Commitment to Health Equity (HCHE) (CY 2025 reporting period/CY 2027 payment or program determination)
Screening for Social Drivers of Health (SDOH) and Screen Positive Rate for SDOH (voluntary reporting for the CY 2025 reporting period)
Beginning in CY 2025, CMS proposes to modify the Immediate Measure Removal policy for adopted OQR and ASCQR Program measures.
Implementation of provisions from the Consolidated Appropriations Act (CAA) of 2023
Medicaid and CHIP
CMS proposes to revise Medicaid and CHIP regulations to codify the requirement that states provide 12 months of continuous eligibility to children under the age of 19.
Non-Opioid Pain Treatment
CMS proposes to implement Section 4135 of the CAA, which will provide temporary additional payments for certain non-opioid pain treatments from January 1, 2025, through December 21, 2027.
CMS states that seven drugs and one device qualify as non-opioid pain treatments and proposes that these products will be separately paid beginning in CY 2025.
CMS requests comments on other products that may qualify.
ADVI will continue monitoring developments and the next steps. This is a delayed release. ADVI Instant content is distributed in real-time for retainer clients. Get in touch to learn more about how we can support your commercialization, market access, and policy needs.